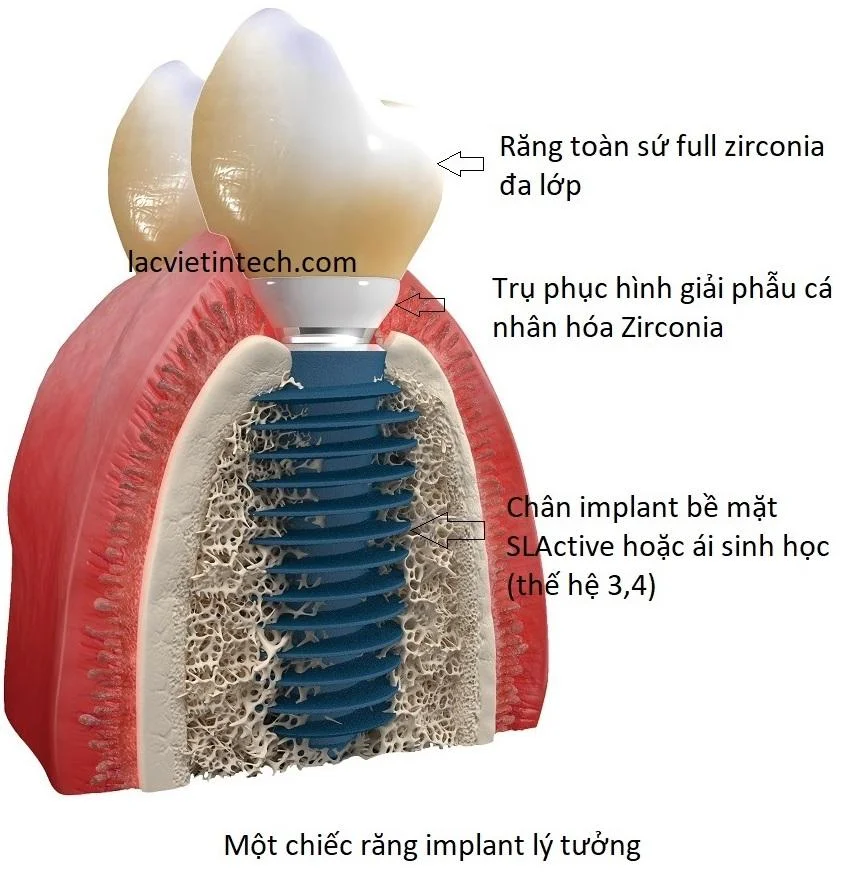
Regarding functionality, every component of a dental implant assumes distinct yet equally critical roles; if just one of the three components is suboptimal, the masticatory function, aesthetics, and longevity of the implant restoration will be compromised.
What is an implant abutment?
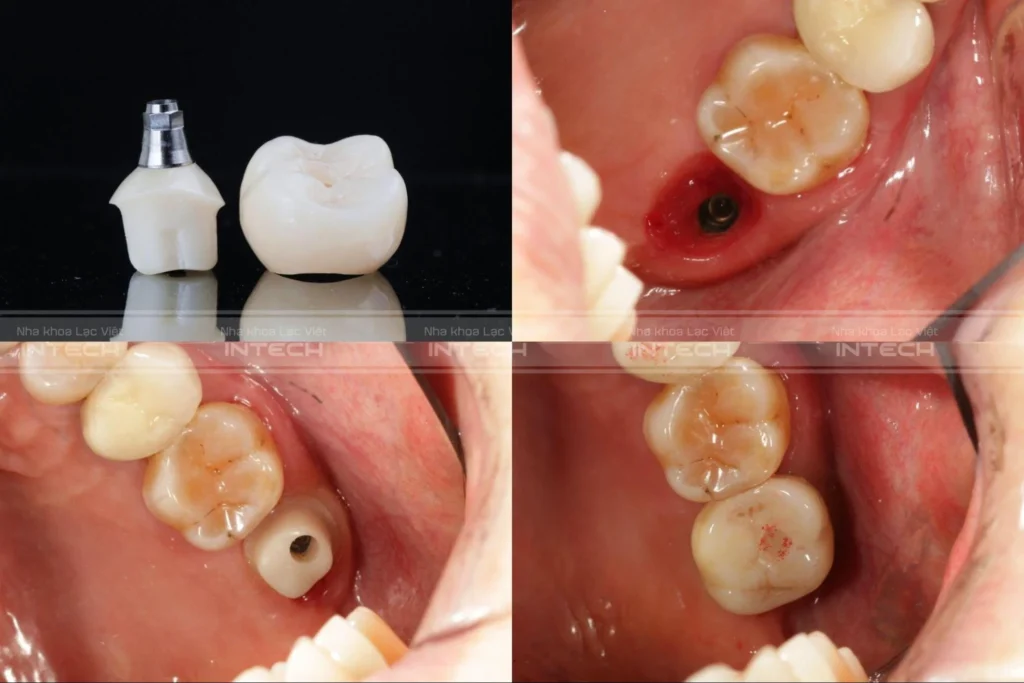
The implant abutment is the component positioned between the prosthetic crown and the artificial tooth root (implant fixture). Structurally, the abutment consists of two parts:
- The subgingival portion (Transmucosal profile): This part resides deep within the gingiva, extending from the implant platform (neck) to the gingival margin, and is referred to as the abutment collar.
- The supragingival portion (Coronal portion): This part protrudes from the gingiva and serves as the retention structure for the prosthetic crown, referred to as the connector.
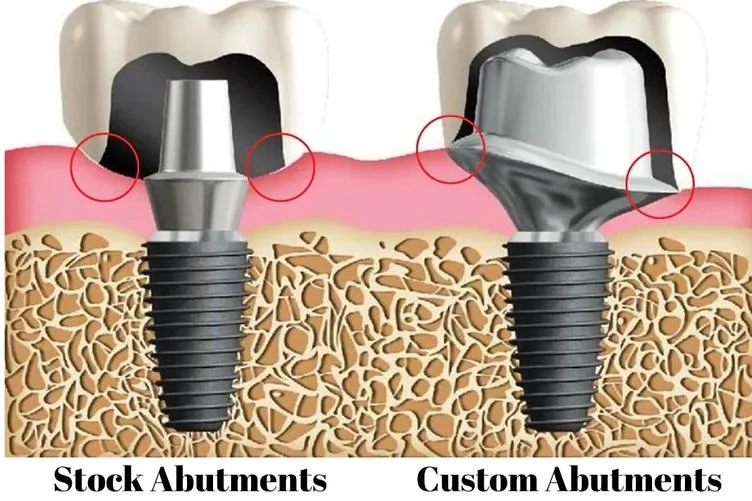
- Image Text:
- Stock Abutments
- Custom Abutments
The abutment comprises two parts: the subgingival portion plays a role in contouring and re-establishing the biology of the gingiva. The portion protruding from the gingiva is the connector, used to attach the porcelain crown.
The Role of the Abutment in Implant Dentistry
The abutment is considered the most critical component in re-establishing aesthetics and sensory perception for the implant restoration. It serves four important roles:
First Role: Aesthetic Reconstruction
The subgingival portion of the abutment is responsible for creating the emergence profile of the implant restoration. Simultaneously, it determines the natural color of the gingiva as well as the natural shade of the overlying ceramic crown. The abutment is the most decisive factor regarding the aesthetics of a dental implant.
Second Role: Establishing a Biological Seal
The subgingival portion of the abutment functions to adhere directly to the gingival tissue, aiming to establish a biological barrier (referred to as the biologic width or seal). This barrier prevents bacteria, food debris, and saliva from the oral environment from invading the underlying implant fixture, thereby ensuring the safety of the implant.
Third Role: Sensory Perception at the Keratinized Gingiva
The subgingival portion of the abutment connects directly with the gingival tissue via creeping attachment or epithelial attachment. Consequently, it transmits masticatory sensations, a degree of taste perception, and food pressure to the gingival tissue. The abutment is the sole component of the implant assembly that participates in sensory reception and food perception.
Fourth Role: Masticatory Load Transmission
The abutment serves as the connection between the intra-bony implant fixture and the intra-oral ceramic crown. When the implant performs masticatory functions (crushing/grinding), occlusal forces from the crown are transmitted through the abutment to the implant fixture, then absorbed and dissipated into the bony trabeculae (Haversian systems) within the jawbone.
Classification of Implant Abutments
An abutment is considered ideal when it satisfies all 5 of the following criteria:
Biological Integration:
Capable of biologically connecting with the gingiva to form a unified entity, creating a solid biological seal to prevent bacteria and external agents (food, thermal changes) from affecting the underlying implant.
Anatomical Reconstruction:
Capable of reconstructing the gingival tissue according to the original anatomical morphology of the lost tooth.
Stability:
High stability to withstand masticatory forces.
Aesthetics:
Does not cause discoloration of the gingiva and/or the overlying ceramic crown.
Sensory Restoration:
Capable of re-establishing food sensation and/or masticatory pressure for the peri-implant gingival tissue.
Based on these 5 criteria, abutments are divided into generations comprising 4 types (within the scope of this article, we do not mention low-quality, low-cost abutments such as Tungsten Stock Abutments or Co-Cr Screw Abutments).

The First Abutment Type: The Generation of Prefabricated (Stock) Abutments
These are abutments mass-produced according to a specific shape (circular cross-section) and a limited range of dimensions. This generation includes 2 types: Cement-retained abutments (Due Abutment or Stock Abutment) and Screw-retained abutments (Screw Abutment or Multi-Unit).
Cement-Retained Abutments (Stock Abutment)
The Stock Abutment is the classic abutment type, emerging alongside the inception of dental implants. Due to cost reasons, cement-retained abutments are still applied in some countries to this day. Stock Abutments possess only a single unique shape—circular—with varying diameters and heights depending on the implant manufacturer, ranging from 4.5mm to 6.5mm in diameter and 5mm to 7mm in height. Cement-retained abutments are fabricated from titanium using casting and sintering technology.

Regarding the connection method to the prosthetic crown, Stock Abutments are bonded to the ceramic crown using an inorganic luting agent such as Glass Ionomer or Fritex.
Precisely because they possess a single shape, limited diameter/height options, are fabricated via casting/sintering, and rely on inorganic cement for retention, cement-retained abutments present multiple disadvantages:
- Inability to reconstruct peri-implant gingival tissue: Because they have only a circular shape, whereas the gingival emergence and cervical profile of each tooth differ (ovoid, parallelogram, trapezoid, etc.).
- Poor stability: Due to fabrication via casting and sintering.
- Gingival discoloration: Can cause darkening of the gingival margin as they are manufactured from titanium, which is black (dark gray).
- Risk of cement sepsis: Excess inorganic cement around the implant can disrupt the biological barrier, causing peri-implantitis.
- Irretrievability: The ceramic crown is cemented permanently to the abutment and cannot be removed for repair if failure occurs.

Due to these numerous disadvantages, cement-retained abutments are increasingly less utilized; the sole reason clinicians select them is their very low cost. From a professional perspective, cement-retained abutments should only be used for provisional restorations while awaiting the final prosthesis.
Screw-Retained Abutments (Screw Abutment)
The Screw Abutment is the second-generation abutment, developed to overcome certain disadvantages of the Stock Abutment. The Screw Abutment is also a prefabricated type manufactured with the same technology as the Stock Abutment, possessing only a single circular shape. However, this type typically has a smaller diameter (usually only two types: 4.5mm and 5.5mm) and fewer dimensional options.
The only difference between the Screw Abutment and Stock Abutment is that the ceramic crown is connected to the Screw Abutment via a screw. Consequently, cement is not required, avoiding cement sepsis and preserving the biological barrier. Furthermore, as the crown is screw-retained, it can be removed for repair if issues arise. However, it still retains the following disadvantages:
- Inability to reconstruct peri-implant gingiva: Due to the single circular shape incompatible with the varied anatomical profiles (ovoid, parallelogram, trapezoid) of natural teeth.
- Poor stability: Due to fabrication via casting and sintering.
- Gingival discoloration: Potential dark gingival margin due to the dark color of titanium.
- Screw loosening: Potential for screw loosening, especially in single-unit restorations.
In practice, Screw Abutments are primarily utilized in full-arch edentulous cases where gingival contouring is not required because a Hybrid denture is employed.
The Second Abutment Type: The Generation of Customized Anatomical Abutments
This is the newest generation of abutments, developed thanks to advancements in material fabrication, CAD/CAM manufacturing technology, and especially Oral Scanning technology. The advent of the Customized Abutment is a significant leap forward in implant dentistry. Specifically, the Zirconia Customized Abutment is considered the final link bringing the implant restoration to perfection.
Unlike the generation of prefabricated abutments, the Customized Abutment is manufactured precisely for each patient and each specific tooth, aiming to create a “prosthetic core” with a morphology identical to a natural tooth core, thereby re-establishing the ideal gingival anatomical profile.
After the implant fixture is placed in the jawbone, the clinician uses Scanning technology to replicate the patient’s teeth and gingiva, then transfers all data to the abutment production center. Here, technicians and doctors design and manufacture an abutment that resembles a natural tooth core, following the exact anatomy of the ideal gingival emergence profile.
Based on the manufacturing material, Customized Abutments are divided into two types: Titanium Customized Abutments and Zirconia Customized Abutments.

Titanium Customized Abutment
Manufactured from titanium using CAD/CAM technology, the Titanium Customized Abutment possesses nearly all the attributes of an ideal abutment, including:
- Biological Integration: Capable of biologically connecting with the gingiva to form a unified entity, creating a solid biological barrier to prevent bacteria and external agents (food, thermal changes) from affecting the underlying implant.
- Anatomical Reconstruction: Capable of reconstructing the gingival tissue according to the original anatomical morphology of the lost tooth.
- High Stability: Capable of withstanding significant masticatory forces as it is produced from monolithic titanium.
- Sensory Restoration: Capable of re-establishing food sensation and/or masticatory pressure for the peri-implant gingiva.
It possesses only one single disadvantage: the dark color of titanium. Therefore, in cases with a thin gingival biotype, it may cause a dark line at the gingival margin, compromising aesthetics.
Zirconia Customized Abutment
The Zirconia Customized Abutment is considered the final link bringing the implant restoration to perfection. Instead of titanium, it is manufactured from Zirconia to overcome the final disadvantage of the Titanium Customized Abutment: the dark gingival margin. Because it is made of white Zirconia, the Zirconia Customized Abutment does not darken the gingival margin like its titanium counterpart.
An absolute advantage of the Zirconia Customized Abutment is its ability to establish a biological barrier. The Zirconia Customized Abutment is capable of forming a biological connection with the gingival tissue via epithelial attachment. This is an extremely robust connection (similar to the attachment of gingiva to the jawbone), capable of absolutely preventing bacterial invasion from the oral environment to the implant fixture below.
The only disadvantage of the Zirconia Customized Abutment is its high cost.

Conclusion:
The ultimate goal of implant dentistry is masticatory function and aesthetics. To fully achieve this goal, the abutment can be considered the most important component of the implant restoration. If a suboptimal abutment is chosen, even if the implant fixture is solid, it cannot provide a beautiful implant tooth that functions without food impaction or chronic inflammation. Therefore, selecting a high-quality abutment is an extremely critical factor when choosing to undergo dental implant treatment.
Related reading for international patients
If you are comparing treatment options, you may also find these guides helpful: Ideal Criteria for a Prosthetic Abutment on Dental Implants, Customized anatomical abutments (customized abutments) and what you need to know and Dental Implant Vietnam: The Complete Guide for International Patients Seeking Safe and Long-Lasting Treatment.
Frequently asked questions
The main types of implant abutments include stock abutments and customized abutments. They differ in shape, fit, aesthetics, and restorative flexibility.
Abutment selection affects soft-tissue support, crown emergence profile, biomechanics, and the long-term stability of the final restoration.
A customized abutment is often preferred when better aesthetics, a more precise emergence profile, or more specific restorative control is needed.
Stock abutments are prefabricated with a standard circular shape, while custom abutments are individually designed using CAD/CAM technology to match the natural tooth anatomy. Custom abutments provide better gum support, aesthetics, and stability.
Zirconia customized abutments are preferred because they are tooth-colored, highly aesthetic, and capable of forming a strong biological seal with the gingiva. They also help prevent dark gum discoloration that may occur with titanium abutments.
Yes. The implant abutment plays a major role in shaping the gum tissue and supporting the crown. A well-designed customized abutment can create a natural emergence profile and improve the overall appearance of the implant restoration.
Customized zirconia abutments are often considered one of the best options for long-term implant restorations because they combine excellent aesthetics, biocompatibility, and precise anatomical design.
Pingback: Ideal Prosthetic Abutment for Dental Implants: Key Clinical Criteria
Pingback: Dental Implant Cost in Vietnam 2026 - Lac Viet Intech Dental Center
Pingback: Customized Anatomic Healing Abutments: A New Trend in Dental Implantology